キーワード:医療連携、健康科学、生命科学、生活習慣病、在宅医療
http://www.tsukuba-igaku-kidney.com/
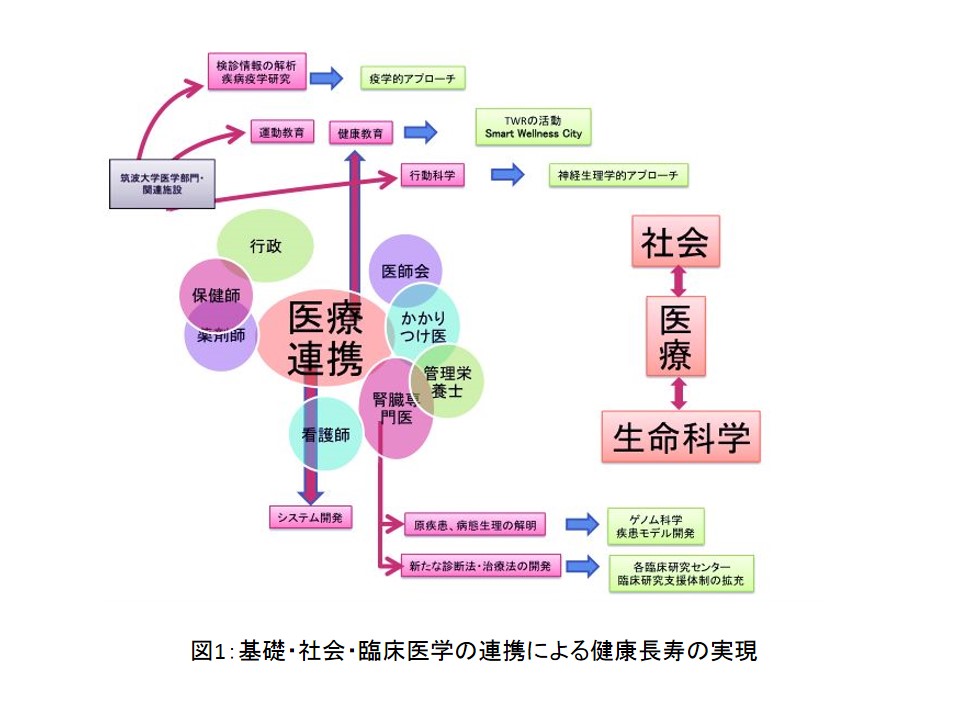
 「CKD(Chronic Kidney Disease=慢性腎臓病」という言葉をご存知でしょうか。日本人の成人人口の約13%、1,330万人がCKD患者となっており、糖尿病をはじめ、呼吸器疾患などを含めた生活習慣病が原因や悪化因子となることが知られ循環器疾患、末期腎不全になる重要なリスクファクターです。CKD患者の診療にはかかりつけ医と腎臓専門医の診療連携が重要であり、治療法の一つとして生活習慣の改善も必要不可欠です。このCKDを中心とした腎疾患・生活習慣病に新しい研 究で立ち向かうリサーチユニットが「基礎・社会・臨床医学の連携による健康長寿の実現」です(図1)。
「CKD(Chronic Kidney Disease=慢性腎臓病」という言葉をご存知でしょうか。日本人の成人人口の約13%、1,330万人がCKD患者となっており、糖尿病をはじめ、呼吸器疾患などを含めた生活習慣病が原因や悪化因子となることが知られ循環器疾患、末期腎不全になる重要なリスクファクターです。CKD患者の診療にはかかりつけ医と腎臓専門医の診療連携が重要であり、治療法の一つとして生活習慣の改善も必要不可欠です。このCKDを中心とした腎疾患・生活習慣病に新しい研 究で立ち向かうリサーチユニットが「基礎・社会・臨床医学の連携による健康長寿の実現」です(図1)。
全国49地区の医師会の協力と連携
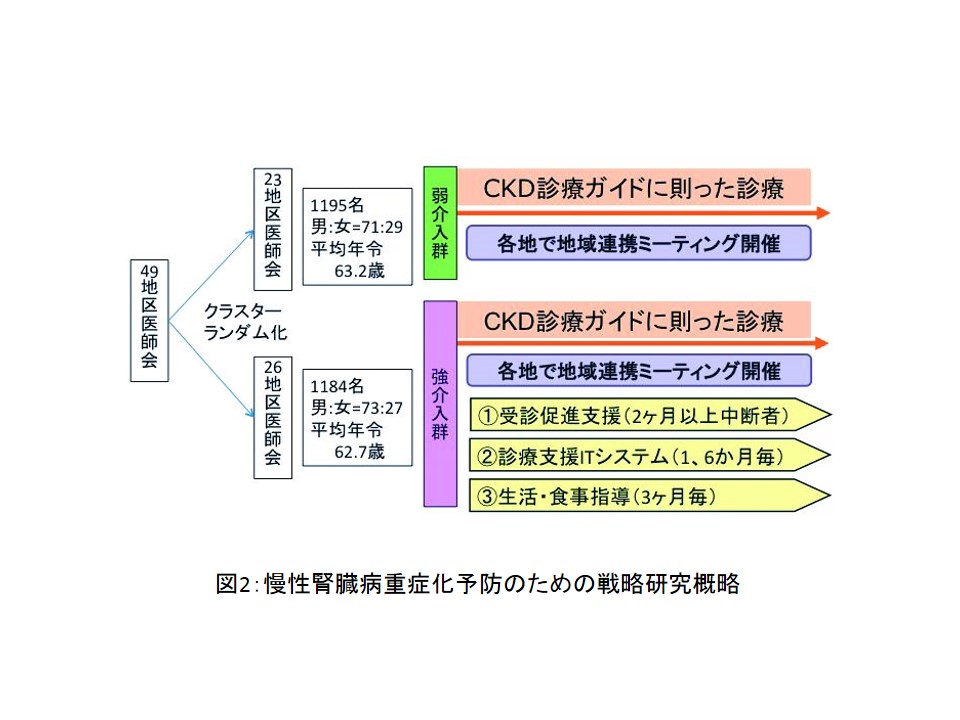
現在取り組んでいる研究は、クラスターランダム化という手法を使い、49地区の医師会の中でかかりつけ医と腎臓専門医の協力を促進して、慢性腎臓病患者において重症化を予防する診療システムの有用性を検討しています。弱介入群と強介入群に分け、強介入群では管理栄養士による生活食事指導を追加し、複数の医療従事者による教育介入の効果について具体的指標を元に評価する研究となっています(図2)。この研究は将来の医療政策に反映させる際に、より実際の診療現場に沿った提言を可能とします。さらに我が国のCKD重症者の入院加療中心の医療から、在宅医療中心の医療へと変貌させることができる可能性を持ち合わせた研究となっています。
CKD予防治療システムの均てん化*1を目指して
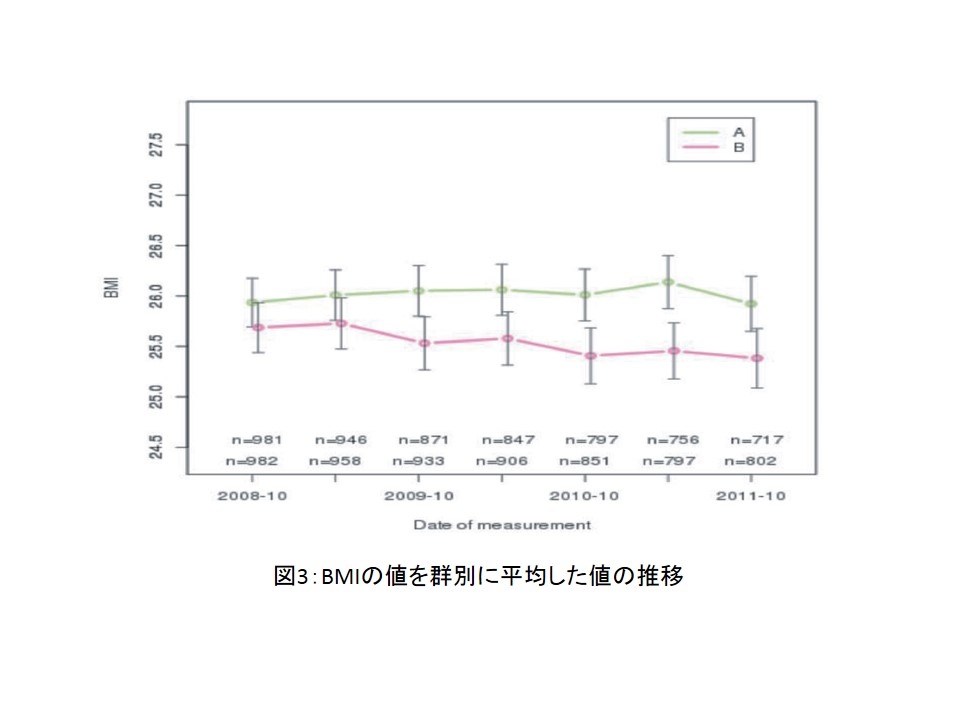
2012年3月までの3.5年の研究結果では強介入群すなわち管理栄養士がついている群は、患者さんが腎臓専門医に受診後、専門医から再びかかりつけ医に戻ってくる割合が高い事が明らかになりました。また、強介入群の患者さんは管理栄養士からの食事指導から体重も減少する割合が高いことも明らかになりました(図3)。今後このような研究成果を生かし、管理栄養士の再教育と共に将来的にこの連携システムの均てん化*を目指し研究を進めていきます。またその中でCKDの早期発見のためのマーカーを発見し今後CKDの予防に役立てていきます。実際に5年後新たに透析を行う患者を15%減らしそれが継続できるように、基礎・社会・臨床研究の融合により、生活習慣に起因するCKDを予防する医療システムを構築するリサーチユニットを目指しています。
*1:均てん化- どこでも標準的な医療を受けられ、地域により医療格差をなくすこと。
社会への貢献・実績
● つくば市、筑波大学、インテル株式会社の三者による地域連携事業の一環として、つくば市民への健康づくりプログラムの提供
● 震災後の福島県伊達市に被災患者の健康管理
● 戦略研究にて得られた研究の成果を検証し、エビデンスを発信し、理想のCKD医療連携の構築
(取材:平成25年9月10日)
‘CKD49’- Approaches to Treat Patients with Chronic Kidney Disease in Cooperation with Medical Associations in 49 districts
Unit members : Usui, Joichi Kondo, Masahide Kai Hirayasu Takahashi, Satoru Shibuya, Akira Ishida, Junji Nakada, Kazuto Nagata, Michio Shimano, Hitoshi Hizawa, Nobuyuki
Key words: medical cooperation, health science, life science, lifestyle-related diseases, home-based care
Do you know the term “chronic kidney disease (CKD)”? Approximately 13% (n=13.3 million) of Japanese adults have CKD. It can be caused or aggravated by lifestyle-related diseases, such as diabetes and respiratory illness, and is an important risk factor for cardiovascular disease and terminal renal failure. To treat CKD patients, cooperation between primary care physicians and nephrologists is important, and it is also crucial to improve their lifestyle. Given this situation, we established a research unit named the “Implementation of Health and Longevity by Cooperation of Basic, Social and Clinical Medical Sciences”, which conducts research on kidney diseases, mainly CKD, and lifestyle-related diseases (Figure 1).

Figure 1: Conceptual diagram of the research unit of the “Achievement of a Healthy and Long Life through Cooperation between Basic Research, Society, and Clinical Medicine”
Cooperation with medical associations in 49 districts in Japan
In our present study, we are investigating the utility of a medical care system aimed at preventing disease progression in CKD patients using a cluster randomization design in cooperation with primary care physicians and nephrologists from medical associations in 49 districts. Specifically, clusters of patients are divided into normal and intense intervention groups, and the latter group receives instructions on lifestyle, including dietary habits, from registered dietitians, and undergoes educational programs provided by multiple healthcare providers. These interventions are evaluated using specific indices (Figure 2). Based on the results of this study, researchers can generate ideas for creating appropriate policies regarding the treatment of CKD. In addition, this study may be able to contribute to shifting from hospital-based to home-based medical care for patients with severe CKD in Japan.

Figure 2: Outline of strategic research to prevent the aggravation of chronic kidney disease
Efforts to achieve the standardization of systems to prevent and treat CKD *1
The results of our study obtained by March 2012, three and a half years after its initiation, revealed that the rate of patients returning to their primary care physicians after consulting nephrologists was higher in the intense intervention group. This group also showed a higher proportion of weight loss owing to dietary instructions provided by registered dietitians (Figure 3). Based on these results, we are going to advance our study with the aim of re-educating registered dietitians and standardizing interprofessional cooperation systems *. We also aim to identify markers of CKD for its early detection and prevention. In addition, to reduce the rate of new dialysis patients by at least 15% in 5 years, and maintain the resultant rate thereafter, our research unit is going to develop medical care systems to prevent lifestyle-related CKD in collaboration with basic research, society, and clinical medicine.
*1: Standardization: Enabling patients to access standard medical care anywhere, and resolving medical disparities between regions

Figure 3: Changes in the average BMI in the normal and intense intervention groups
Social contributions and achievements
● Implementation of programs to promote the health of residents of Tsukuba City as one of the regional cooperation projects organized by the city, University of Tsukuba, and Intel Corporation
● Management of the health of patients living in Date City, Fukushima Prefecture, who were affected by the Great East Japan Earthquake
● Verification of the results of strategic research, the publication of evidence supporting these results, and the establishment of favorable CKD-related medical cooperation